Pain is a normal experience
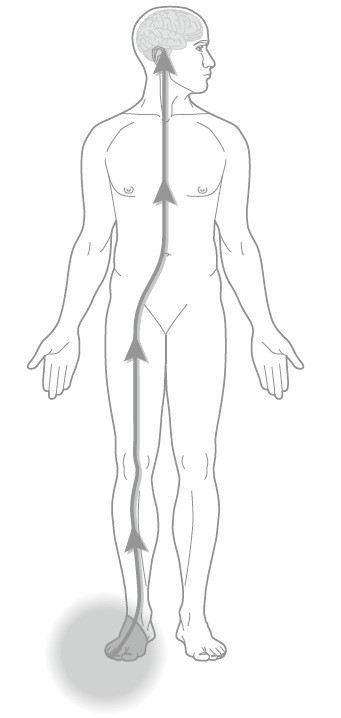 Pain is a normal, but unpleasant, experience you feel in response to what your brain believes to be a threatening situation and can involve actual or potential tissue damage (Butler & Moseley, 2003). The pain experience is what motivates you to take notice of tissue damage and do something about it. When you accidentally step on a sharp object your brain alerts you to the threat (tissue damage) and you will quickly remove your foot from the object to prevent further damage. Think of your pain as an alarm system; it has the capability of sending danger messages to your brain when your brain perceives that it is under threat. Your brain then processes these danger messages and decides what the necessary action your body should take to prevent further tissue damage (like removing your foot from that sharp object). This system is essential to your survival.
Pain is a normal, but unpleasant, experience you feel in response to what your brain believes to be a threatening situation and can involve actual or potential tissue damage (Butler & Moseley, 2003). The pain experience is what motivates you to take notice of tissue damage and do something about it. When you accidentally step on a sharp object your brain alerts you to the threat (tissue damage) and you will quickly remove your foot from the object to prevent further damage. Think of your pain as an alarm system; it has the capability of sending danger messages to your brain when your brain perceives that it is under threat. Your brain then processes these danger messages and decides what the necessary action your body should take to prevent further tissue damage (like removing your foot from that sharp object). This system is essential to your survival.
Pain is a poor marker for tissue damage
We already know that pain can be related to a change in your tissues. Postural pains, pains from a sprained ankle, and pain from a bulging disc are all the result of some degree of damage to the surrounding tissues. You would assume that the larger the degree of tissue damage, the greater degree of pain. So, why is a paper cut on a finger so painful? Why are migraines so debilitating?
What we now understand is that the severity of the pain report does not always give an accurate indication of the degree of tissue damage. Paper cuts on a finger typically involve only a minor amount of tissue damage (which heals with little or no care on your part), but the degree of your pain report is usually quite high, while some life threatening cancers can go undetected for years as there are no associated symptoms. This highlights our understanding that pain is a much more complex phenomenon than we expected.
When pain becomes persistent
Whenever we injure ourselves, the damage to the surrounding tissues activates a cascade of events known as inflammation. Inflammation helps to promote healing of your tissues. Different tissues take different amounts of time to heal, but typically, all tissues do heal. We expect that as the tissue heals, the degree of pain associated will lessen over time. So, why do some people report ongoing or increasing pain symptoms that last months to years, well beyond the expected healing time for the injured tissue?
There is no easy answer to this question. There may be some ongoing inflammatory reactions in the tissues that cause the persisting pain. The tissues may have healed but are not yet healthy; muscles may remain weak and underused, there may be motor control issues with the core muscles. Or, the central nervous system (brain and spinal cord) may have become sensitized over time. Essentially, this system becomes too good at what it does. This can involve the following:
- Neurons in the spinal cord become more sensitive and more efficient at sending danger messages from the tissues to the brain, thereby magnifying the danger message your brain receives.
- The virtual representation of the affected limb (homunculus) in the brain is enlarged. This is an adaptation to the persistent pain; your brain will pay more attention to the affected area.
- Smudging can occur in the outer cortex of the brain, which results in overlapping of the brain areas devoted to certain areas of the body. This can result in the sensation that the pain is spreading to adjacent body parts.
- Negative thoughts (“there is something seriously wrong with me”, “there is nothing I can do about the pain”) can act like nerve impulses.
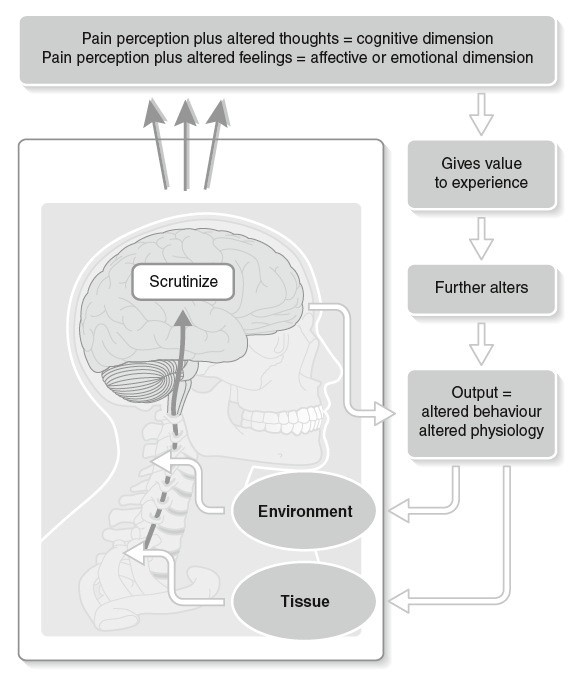
Reproduced from Lee D 2011 The Pelvic Girdle, 4th edn with permission
These changes result in central sensitization. The central nervous system (CNS) becomes like the oversensitive smoke detector in your home, which goes off when you burn birthday candles or burn your toast. The smoke detector works, but it is too sensitive and providing you too much, and often unnecessary, information.
In a centrally sensitized state, the brain receives magnified danger messages from the spinal cord. The brain then prioritizes all these messages and decides what is the most urgent action to take. It has the capability of activating a number of systems to take what it believes to be the necessary action. It can call upon the motor system to get you to fight or move away from the situation (e.g. taking your foot off that sharp object) or splint/brace a damaged area. The pain system can be activated to get you to take notice and do something about it. It can activate the sympathetic nervous system, which results in increased heart rate, sweating, and increased vigilance. A number of systems can be triggered (endocrine, immune, parasympathetic as well); your brain decides at that moment based on the information it is receiving from the spinal cord.
Management strategies
There are a number of management tools and strategies that you can take to address persistent pain issues. It is important to start with a thorough assessment by a health care professional(s) to help gain a better understanding of your situation. With this information, there will be a better understanding of what it is that is perpetuating your pain state – ongoing tissue problems, sensitized nervous system, or both. From there, management can include the following:
- Education on your pain states: In order to learn how to better manage pain, it is important for those living with persistent pain to better understand the physiology behind what is driving the ongoing pain. Although concepts of central sensitization seem complex, we know that patients do have the ability to understand them with only brief amounts of education from a trained professional (Moseley, 2003). Intensive education on pain neurophysiology, with no concurrent physical treatment, has also been shown to increase one’s perception that they can control their pain and can increase some physical measures (straight leg raise, forward bend) in those with persistent low back pain (Moseley et al., 2004). Another study also showed a general reduction in cortical brain activity during an abdominal cue to activate transversus abdominis (TrA) in a patient with chronic low back pain following 1:1 education on pain neurophysiology (Moseley, 2004). This marked reduction in brain activity was not seen on scanning following intensive practice of the TrA activation alone but was noted only after the education on persistent pain. This highlights that a better understanding of the persistent pain state can decrease the threat value of a physical task, helping to “unwind” the sensitized CNS.
- Pacing & Graded Exposure: In some instances following an injury, negative beliefs and a fear of (re)injury can result in poor coping mechanisms, excessive guarding, and overprotective behaviors that can perpetuate the pain problem. This can then result in avoidance of a particular activity/movement that you feel is threatening (for example, someone who was injured falling down a flight of stairs may avoid stairs later on due to their fear of falling and reinjuring themselves). Early on in your treatment, it is important to work with your physiotherapist to first determine what activity you are avoiding due to your fear of (re)injury. You can then work together to establish your baseline for that activity; in other words, what is the degree to which you can participate in that activity without flaring up your pain in such a way that it can take hours/days to settle back down. With your physiotherapist, you can then establish an approach to gradually increase your tolerance for the activity in such a way that you continue to avoid flare ups of your pain. This is a graded exposure approach to treatment. Recent studies have shown that a graded exposure approach to the threatening activity/movement can decrease one’s level of pain-related fear, pain disability, and pain intensity in those diagnosed with chronic pain disorders (de Jong et al., 2005). This treatment approach has also been shown to significantly reduce measures on fear of pain/movement and pain-related anxiety in those with chronic low back pain (Woods & Asmundson, 2008).
- Treat the impairment: It is crucial in management of chronic pain issues to understand the physiology behind the hypersensitive CNS; however, it is still important to address any underlying physical impairment. Along with the above treatment, it is important to work with your physiotherapist to treat any underlying physical issues (e.g. motor control issues, lack of joint mobility, loss of muscle strength). Treatment will focus on improving your function in such a way that your pain symptoms are not flared up as a consequence. You should work with your physiotherapist to design a unique treatment program that addresses your pain issues and physical impairments. This may also include other health care professionals, like your family doctor, psychologist, and/or specialist(s). Treatment may also include counselling around pain management, medication(s), diaphragmatic breath training/capnography etc. It is important for you to have a good understanding of your treatment plan and goals and for you to take a shared responsibility in the management of your persistent pain issues.
References
Butler, D & Moseley, L. Explain Pain. Noigroup Publications; 2003.
de Jong, J.R. et al. (2005). Reduction of pain-related fear in complex regional pain syndrome type 1: The application of graded exposure in vivo. Pain, 116: 264-275.
Lee D G (2011). The Pelvic Girdle, 4th edn. Elsevier, Edinburgh
Moseley, Lorimer. (2003): Unraveling the Barriers to Reconceptualization of the Problem in Chronic Pain: The Actual and Perceived Ablity of Patients and Health Professionals to Understand the Neurophysiology. Journal of Pain, 4(4): 184-189
Moseley, L.G., et al. (2004): A Randomized Controlled Trial of Intensive Neurophysiology Education in Chronic Low Back Pain. Clinical Journal of Pain, 20: 324-330.
Moseley, L. (2004): Widespread brain activity during an abdominal task markedly reduced after pain physiology education: fMRI evaluation of a single patient with chronic low back pain . Australian Journal of Physiotherapy. 51: 49-52.
Woods, M.P & Asmundson, G. (2008): Evaluating the efficacy of graded in vivo exposure for the treatment of fear in patients with chronic back pain: A randomized controlled clinical trial. Pain, 136: 271-280.
Related Services


The Integrated Systems Model
This model allows clinicians to be more effective and efficient with their assessment and treatment in order to help patients develop better movement strategies and habits to help reduce symptoms and improve function and performance.



